Depending on the dosage, the person and the setting, the effects can manifest as changes in mood, perception and cognition, which are also known as Altered States of Consciousness (ASC). These are characterised by visual and mental hallucinations, a distorted sense of time, increased sensory experiences, synaesthesia, disorientation, lethargy, and an enhanced ability for introspection [12]. This list is non-exhaustive.
In general, the physiological side effects are not significant and may include pupil dilation (93%); changes in heart rate (100%), including increases (56%), decreases (13%), and variable responses (31%); changes in blood pressure (84%), including hypotension (34%), hypertension (28%), and general instability (22%); changes in stretch reflex (86%), including increases (80%) and decreases (6%); nausea (44%); tremor (25%); and dysmetria (16%) [8].
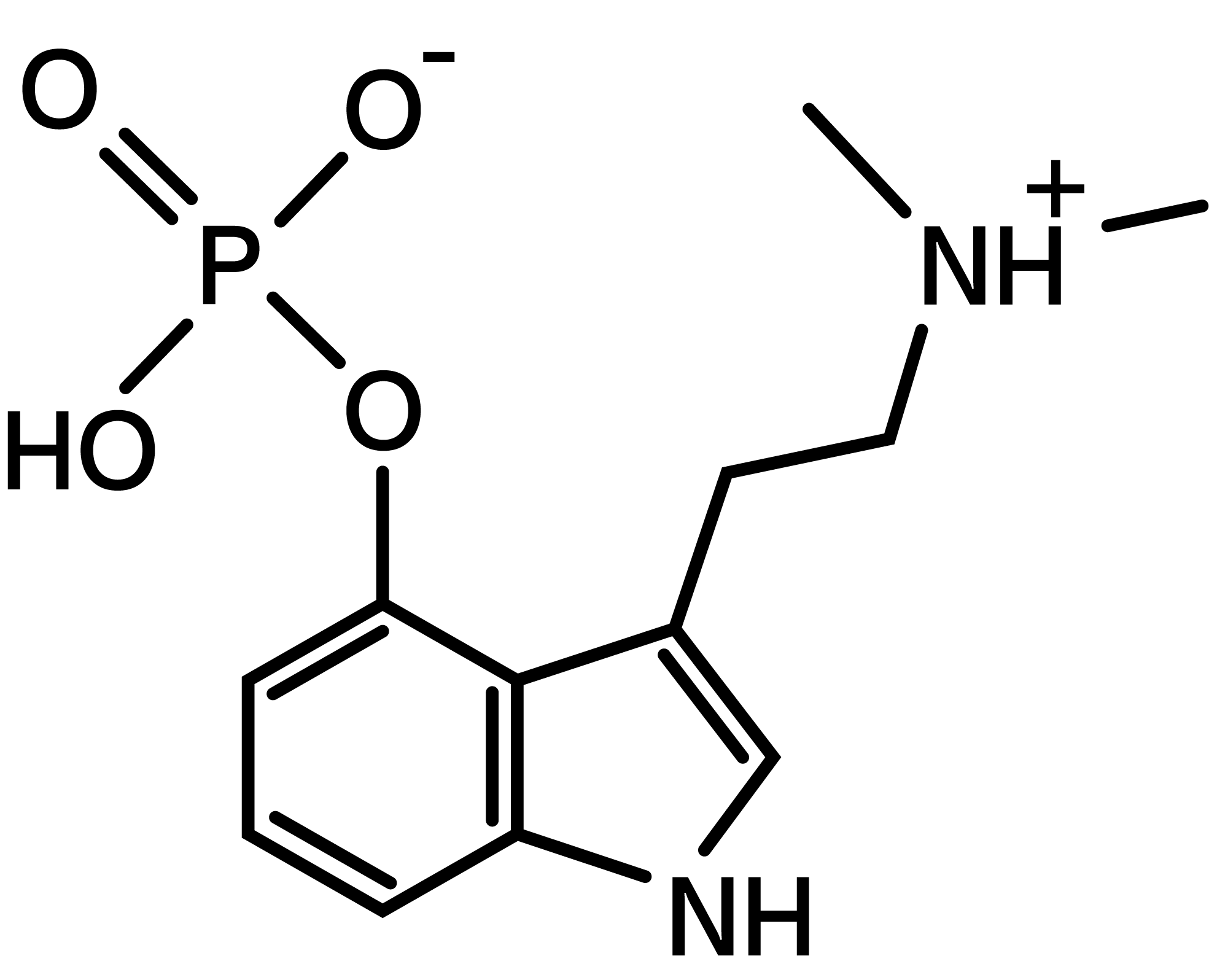
Psilocybin (4-PO-HO-DMT) is the phosphorylated form of psilocin (4-HO-DMT), the actual psychoactive compound, which is also found in magic mushrooms, albeit in lower concentrations. After ingestion, psilocybin is rapidly converted to its active metabolite psilocin.
Both substances can be found in the majority of so-called magic mushrooms. There are about 200 species of psilocybin fungi, which belong in particular to the Psilocybe, Panaeolus and Conocybe genus [10]. Other genera of mushrooms that produce psilocybin are Gymnopilus, Inocybe, Paneolus, Photoliotina and Pluteus. Magic mushrooms are usually ingested orally, either fresh or dried, mixed into foods or made into tea.
In scientific research, pure psilocybin is typically preferred to magic mushrooms, given that it is more stable and because other compounds in these mushrooms may confound results or lead to adverse reactions [11]. For this reason, there might be a difference between ingesting Magic Mushrooms and pure psilocybin. Do read our blog article here if you want to know more about this specific topic.
Psilocin mostly acts as a partial agonist (activator) on the 5-HT1A/5-HT2 receptors, more specifically the 5-HT2A, 5-HT2B and 5-HT2C receptors [8]. The psychedelic effect is dependent on 5-HT2A [c] activity, but the mechanism underlying the long-term therapeutic effect in depressed patients is still unclear [9, 13, 14]. Neuronal plasticity has been proposed to play a role in this long-term effect of psilocybin and other psychedelics [9]. Through activation of 5-HT2A receptors, psilocybin may promote the release of brain-derived neurotrophic factor, which in turn could contribute to its long-lasting effects [9].
In a review by Van Amsterdam and colleagues in 2011, it was concluded that the use of magic mushrooms rarely (if ever) leads to physical or psychological dependence, that acute and chronic adverse effects are relatively infrequent and generally mild, that the effects on public health and public order are very limited and that criminality related to the use, production and trafficking of magic mushrooms is almost non-existent [15].
However, the authors specified that attention should be paid to the infrequent occurrence of accidents and flashbacks, particularly in the absence of proper surveillance of the user [15]. Magic mushroom use can evoke panic attacks, and while this is rare, can lead to severe, and sometimes fatal accidents [15]. High places and water should be avoided. The same authors conclude that accidents can be prevented by a supportive setting with surveillance by a sober person.
In the context of clinical trials, single or few doses of psilocybin seem to be well tolerated [16].
Physical risks
The toxicity of psilocybin is low. Based on the results of animal studies, the lethal dose of pure psilocybin has been extrapolated to be 6 grams, 240 times greater than the typical dose of 25 mg that is used in clinical trials [6].
To achieve these levels through the oral consumption of magic mushrooms, extreme amounts would need to be ingested, which would induce stomach pain, persistent vomiting, and diarrhoea. These effects are not caused by psilocybin/psilocin, but by the other compounds found in these mushrooms [15].
While body temperature typically remains normal, a temporary increase in heart frequency and blood pressure can occur [15]. The most likely cause of this adverse reaction is phenylethylamine, another compound in magic mushrooms. It entails a risk for users with pre-existing cardiovascular conditions [11].
Interaction of magic mushrooms with other drugs
When fatalities occur after the consumption of magic mushrooms, they are often due to the combination with other drugs, typically alcohol [15].
Alcohol can increase the production of metabolites that inhibit mono-amino oxidase (MAO) enzymes. Since these enzymes contribute to the biological inactivation of psilocybin, psilocin and other magic mushroom compounds, their inhibition could explain why alcohol may enhance the (adverse) effects induced by magic mushrooms [15].
Chocolate also contains MAO-inhibitors, but the amount of MAO-inhibitors in regular chocolate is clinically not relevant [15].
Finally, tobacco use is associated with lowered levels of MAO in the brain and peripheral organs. Smokers may therefore experience more pronounced (adverse) effects of magic mushrooms compared to non-smokers [15].
Addiction
Psilocybin or psilocin are not physically or psychologically addictive [8].
Flashbacks
Often cited dangers of psychedelic drug use include Hallucinogen Persisting Perception Disorder (HPPD), psychosis, and “flashback” phenomena [17-19].
A 2003 review of 20 quantitative studies that focused on HPPD concluded that very little was known about this condition [20]. In a more recent 2010 study, a sample of 503 recreational psilocybin users, 4 participants (0.8%) spontaneously reported symptoms of HPPD, but none of the participants reported flashbacks [21]. Nevertheless, the risk of prolonged psychoses may be lower in a controlled setting, and fewer psychotic symptoms are reported with non-patient groups (0.08%) compared to a patient group (0.2%) [22].
Given that psilocybin induces a state that mimics certain aspects of acute and developing stages of schizophrenia [23- 27], the possible role of hallucinogens in precipitating or exacerbating (lasting) psychosis, other psychiatric conditions, and long-lasting visual perceptual disturbances should be assessed more closely [15].
In schizophrenic patients, the consumption of magic mushrooms may induce an acute psychotic state that necessitates hospitalization [28].
There have been multiple mushroom-like primitive cave paintings, carvings, and sculptures discovered around the world. These artefacts could be evidence of early primitive use of psilocybin-containing mushrooms but there is no consensus among researchers.
The oldest examples are the rock paintings of the Tassili-n-Ajjer Plateau in Alegria. These paintings date back from the late Neolithic period to 1000 BC and onward. A figure can be seen with what seems like fists full of mushrooms and sprouting mushrooms from the arms and legs [29- 31].
After this, there are colonial accounts of Spanish missionaries describing the ritual and/or medicinal use of psychedelic mushrooms by native Americans in the 17th century [32]. In the 1930’s, a botanist named Richard Evans Schultes pioneered studies of shamanistic mushroom use in Mexico.
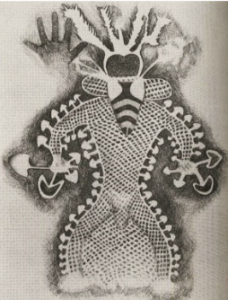 Figure 1
Figure 1
Figure 2
 Figure 3
Figure 3
The modern history and popularity of psilocybin and psilocybin containing mushrooms in the US and Europe began in the early 1950s, when amateur ethnomycologist Robert Gordon Wasson and his wife Valentina Pavlovna studied and experienced the ritual use of mushrooms in the Mazatec village of Huautla de Jiménez in Mexico.
They were introduced to these sacred mushroom ceremonies, Veladas, by María Sabina. She was the first Curandera, a Mazatec shaman or healer, who allowed westerners to participate in these rituals.
The publicity that followed Watson’s publications caused an influx of Westerners wanting to experience the mushroom-induced hallucinations. This unwanted attention caused problems in the dynamics of the community. Sabina was ostracized and her house was burned down. She later regretted having introduced Wasson to the practice [33].
On one of his expeditions, Wasson took along French mycologist Roger Heim, who afterwards managed to grow the mushrooms in his laboratory at the Natural History Museum in Paris. In 1958, he sent samples to the chemist Albert Hofmann, who invented LSD. Hofmann managed to isolate psilocybin and later synthesize it in his laboratory.
The Swiss pharmaceutical company, Sandoz, where Hofmann worked, marketed psilocybin under the name Indocybin, and sold it to doctors and psychiatrists around the world for experimental use.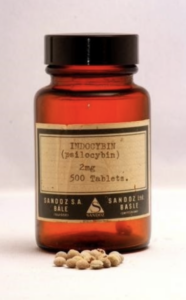
Two of the most famous pioneering studies on psilocybin were the Concord Prison Experiment and the Marsh Chapel Experiment. The first was conducted between 1961 and 1963 at the high-security prison in Concord, Massachusetts, USA, by a team of Harvard researchers led by Dr. Timothy Leary. The study aimed to assess the effects of psilocybin-assisted psychotherapy on the recidivism rate of convicts. The initial results showed promise [34], but a subsequent review revealed methodological biases that questions these positive results [35].
In the Marsh Chapel Experiment, also called the Good Friday experiment, psychiatrist and theologian Walter Pahnke administered psilocybin to a group of divinity students at the Good Friday Mass at Boston University’s Marsh Chapel in 1962. The aim was to see if psilocybin could elicit true mystical experiences. As with the Concord study, the reported results were positive, but again, a follow-up study [36] conducted 25 years later, found some methodological weaknesses, but did not question the overall results of the study. Most participants remembered the experience as one of the most important events of their lives. One of the subjects, the theologian Huston Smith, later became a leading author on religious issues, and a staunch defender of the idea that the mystical experiences elicited by psychedelics are not distinct from those that arise spontaneously [36, 37].
The first bans on psilocybin were implemented in 1966 in the United States, at the same time as the bans on LSD. By the 1970’s, research into psilocybin, and psychedelics in general, had come to a halt. These bans occurred during the Nixon administration, and were part of “the War on Drugs” [38].
In June 2011, the Global Commission on Drug Policy declared that “The global war on drugs has failed, with devastating consequences for individuals and societies around the world. Fifty years after the initiation of the UN Single Convention on Narcotic Drugs, and years after President Nixon launched the US government’s war on drugs, fundamental reforms in national and global drug control policies are urgently needed.” [39]
Since the revival of psychedelic research in the early 1990’s, psilocybin has been one of the most popular substances in scientific studies. Researcher Matthew Johnson explains that this is due to several contributing factors. Firstly, it already had a well-established background in basic toxicology and pharmacology, because it was one of the most studied classical psychedelic substances on human subjects during the 1950s and 1960s. Therefore it did not need to go through the many basic safety studies, as would be the case with a new compound. Secondly, its five- to six-hour duration of effects is more convenient in a professional context, compared to the ten to twelve hours of LSD and mescaline. And last but not least, it is far less politically sensitive than LSD, which is often still linked with the sixties’ counter culture [40].
Recent and ongoing research on Psychedelic-Assisted Therapy with psilocybin, focuses on end-of-life anxiety, post-traumatic stress disorder (PTSD), tobacco and alcohol addiction, depression, obsessive-compulsive disorder (OCD) and cluster headaches, but also the ability of this substance to boost creativity and elicit mystical experiences [41].
[1] Nicholas CR, Henriquez KM, Gassman MC, et al. High dose psilocybin is associated with positive subjective effects in healthy volunteers. J Psychopharmacol. 2018;32(7):770-778. doi:10.1177/0269881118780713
[2] Malone TC, Mennenga SE, Guss J, et al. Individual Experiences in Four Cancer Patients Following Psilocybin-Assisted Psychotherapy. Front Pharmacol. 2018;9:256. Published 2018 Apr 3. doi:10.3389/fphar.2018.00256
[3] Brown RT, Nicholas CR, Cozzi NV, et al. Pharmacokinetics of Escalating Doses of Oral Psilocybin in Healthy Adults. Clin Pharmacokinet. 2017;56(12):1543-1554. doi:10.1007/s40262-017-0540-6
[4] F. Hasler, D. Bourquin, R. Brenneisen, T. Bär, F.X. Vollenweider, Determination of psilocin and 4-hydroxyindole-3-acetic acid in plasma by HPLC-ECD and pharmacokinetic profiles of oral and intravenous psilocybin in man, Pharmaceutica Acta Helvetiae, Volume 72, Issue 3, 1997, Pages 175-184, ISSN 0031-6865, https://doi.org/10.1016/S0031-6865(97)00014-9.
[5] Hasler F, Grimberg U, Benz MA, Huber T, Vollenweider FX. Acute psychological and physiological effects of psilocybin in healthy humans: a double-blind, placebo-controlled dose-effect study. Psychopharmacology (Berl). 2004;172(2):145-156. doi:10.1007/s00213-003-1640-6
[6] Gable RS. Comparison of acute lethal toxicity of commonly abused psychoactive substances. Addiction. 2004;99(6):686-696. doi:10.1111/j.1360-0443.2004.00744.x
[7] Stenbæk DS, Madsen MK, Ozenne B, et al. Brain serotonin 2A receptor binding predicts subjective temporal and mystical effects of psilocybin in healthy humans. J Psychopharmacol. 2021;35(4):459-468. doi:10.1177/0269881120959609
[8] Passie T, Seifert J, Schneider U, Emrich HM. The pharmacology of psilocybin. Addict Biol. 2002;7(4):357-364. doi:10.1080/1355621021000005937
[9] Aleksandrova LR, Phillips AG. Neuroplasticity as a convergent mechanism of ketamine and classical psychedelics. Trends Pharmacol Sci. 2021;42(11):929-942. doi:10.1016/j.tips.2021.08.003
[10] Wikipedia Contributors. List of psilocybin mushroom species. Wikipedia. Published November 12, 2019. Accessed December 2, 2019. https://en.wikipedia.org/wiki/List_of_psilocybin_mushroom_species
[11] Beck O, Helander A, Karlson-Stiber C, Stephansson N. Presence of phenylethylamine in hallucinogenic Psilocybe mushroom: possible role in adverse reactions. J Anal Toxicol. 1998;22(1):45-49. doi:10.1093/jat/22.1.45
[12] Hirschfeld T, Schmidt TT. Dose-response relationships of psilocybin-induced subjective experiences in humans. J Psychopharmacol. 2021;35(4):384-397. doi:10.1177/0269881121992676
[13] Hesselgrave N, Troppoli TA, Wulff AB, Cole AB, Thompson SM. Harnessing psilocybin: antidepressant-like behavioral and synaptic actions of psilocybin are independent of 5-HT2R activation in mice. Proc Natl Acad Sci U S A. 2021;118(17):e2022489118. doi:10.1073/pnas.2022489118
[14] De Gregorio D, Aguilar-Valles A, Preller KH, et al. Hallucinogens in Mental Health: Preclinical and Clinical Studies on LSD, Psilocybin, MDMA, and Ketamine. J Neurosci. 2021;41(5):891-900. doi:10.1523/JNEUROSCI.1659-20.2020
[15] van Amsterdam J, Opperhuizen A, van den Brink W. Harm potential of magic mushroom use: a review. Regul Toxicol Pharmacol. 2011;59(3):423-429. doi:10.1016/j.yrtph.2011.01.006
[16] Dos Santos RG, Bouso JC, Alcázar-Córcoles MÁ, Hallak JEC. Efficacy, tolerability, and safety of serotonergic psychedelics for the management of mood, anxiety, and substance-use disorders: a systematic review of systematic reviews. Expert Rev Clin Pharmacol. 2018;11(9):889-902. doi:10.1080/17512433.2018.1511424
[17] COHEN S, DITMAN KS. Prolonged adverse reactions to lysergic acid diethylamide. Arch Gen Psychiatry. 1963;8:475-480. doi:10.1001/archpsyc.1963.01720110051006
[18] Novak SJ. Second thoughts on psychedelic drugs. Endeavour. 1998;22(1):21-23. doi:10.1016/s0160-9327(98)01096-5
[19] Johnson M, Richards W, Griffiths R. Human hallucinogen research: guidelines for safety. J Psychopharmacol. 2008;22(6):603-620. doi:10.1177/0269881108093587
[20] Halpern JH, Pope HG Jr. Hallucinogen persisting perception disorder: what do we know after 50 years?. Drug Alcohol Depend. 2003;69(2):109-119. doi:10.1016/s0376-8716(02)00306-x
[21] Carhart-Harris RL, Williams TM, Sessa B, et al. The administration of psilocybin to healthy, hallucinogen-experienced volunteers in a mock-functional magnetic resonance imaging environment: a preliminary investigation of tolerability. J Psychopharmacol. 2011;25(11):1562-1567. doi:10.1177/0269881110367445
[22] COHEN S. Lysergic acid diethylamide: side effects and complications. J Nerv Ment Dis. 1960;130:30-40. doi:10.1097/00005053-196001000-00005
[23] Carter OL, Burr DC, Pettigrew JD, Wallis GM, Hasler F, Vollenweider FX. Using psilocybin to investigate the relationship between attention, working memory, and the serotonin 1A and 2A receptors. J Cogn Neurosci. 2005;17(10):1497-1508. doi:10.1162/089892905774597191
[24] Hasler F, Grimberg U, Benz MA, Huber T, Vollenweider FX. Acute psychological and physiological effects of psilocybin in healthy humans: a double-blind, placebo-controlled dose-effect study. Psychopharmacology (Berl). 2004;172(2):145-156. doi:10.1007/s00213-003-1640-6
[25] Vollenweider FX, Vollenweider-Scherpenhuyzen MF, Bäbler A, Vogel H, Hell D. Psilocybin induces schizophrenia-like psychosis in humans via a serotonin-2 agonist action. Neuroreport. 1998;9(17):3897-3902. doi:10.1097/00001756-199812010-00024
[26] Gouzoulis-Mayfrank E, Habermeyer E, Hermle L, Steinmeyer A, Kunert H, Sass H. Hallucinogenic drug induced states resemble acute endogenous psychoses: results of an empirical study. Eur Psychiatry. 1998;13(8):399-406. doi:10.1016/S0924-9338(99)80686-5
[27] Vollenweider FX, Geyer MA. A systems model of altered consciousness: integrating natural and drug-induced psychoses. Brain Res Bull. 2001;56(5):495-507. doi:10.1016/s0361-9230(01)00646-3
[28] Nielen RJ, van der Heijden FM, Tuinier S, Verhoeven WM. Khat and mushrooms associated with psychosis. World J Biol Psychiatry. 2004;5(1):49-53. doi:10.1080/15622970410029908
[29] Drawing by Kat Harrison-McKenna. From O. T. Oss and O.N. Oeric, Psilocybin, The Magic Mushroom Grower’s Guide,1986, p. 71. From the original in Jean-Dominique Lajoux, The Rock paintings of the Tasilli (New York: World Publishing, 1963), p.71.
[30] Winkelman, M. J. (2021). The Evolved Psychology of Psychedelic Set and Setting: Inferences Regarding the Roles of Shamanism and Entheogenic Ecopsychology. Frontiers in Pharmacology, 12, 619890–619890. https://doi.org/10.3389/fphar.2021.619890
[31] De Borhegyi, C., & de Borhegyi-Forrest, S. (2015). Chapter 11 – Mushroom Intoxication in Mesoamerica. In History of Toxicology and Environmental Health (pp. 104–115). Elsevier Inc. https://doi.org/10.1016/B978-0-12-801506-3.00011-X
[32] Bibliography 1.Plants of mind and spirit – teonanacatl mushrooms. Fed.us. Accessed October 19, 2021. https://www.fs.fed.us/wildflowers/ethnobotany/Mind_and_Spirit/teonanacatl.shtml
[33] Estrada, Álvaro, (1976) Vida de María Sabina: la sabia de los hongos (ISBN 968-23-0513-6)
[34] Erowid Tim Leary vault : Concord prison psilocybin rehabilitation project. Erowid.org. Accessed October 19, 2021. https://www.erowid.org/culture/characters/leary_timothy/leary_timothy_concord_prison1.shtml
[35] Doblin R. Dr. Leary’s Concord Prison Experiment: a 34-year follow-up study. J Psychoactive Drugs. 1998;30(4):419-426. doi:10.1080/02791072.1998.10399715
[36] Doblin R., Pahnke’s “Good Friday Experiment” : A Long-Term Follow-Up And Methodological Critique, 1991; The Journal of Transpersonal Psychology, Vol 23, No 1.
[37] Horgan J. R.I.p. huston smith, religious scholar who defended psychedelics’ spiritual potential. Scientificamerican.com. Accessed October 19, 2021. https://blogs.scientificamerican.com/cross-check/r-i-p-huston-smith-religious-scholar-who-defended-psychedelics-spiritual-potential/
[38] Wikipedia contributors. War on drugs. Wikipedia, The Free Encyclopedia. Published October 10, 2021. Accessed October 19, 2021. https://en.wikipedia.org/w/index.php?title=War_on_drugs&oldid=1049124510
[39] War on Drugs. The Global Commission on Drug Policy. 2011. p. 24. Archived from the original on January 9, 2016. Retrieved September 18, 2017
[40] Roes T. [Interview] Matthew Johnson: “Psychedelic therapy may become available in a decade.” Stichtingopen.nl. Accessed October 19, 2021. https://www.stichtingopen.nl/matthew-johnson-psychedelic-therapy-may-become-available-decade/
[41] Pollan, M. 2019. How to Change Your Mind: The New Science of Psychedelics. Harlow, England: Penguin Books.